


What if there were a type of eating disorder that medical professionals frequently did not recognize, and had little knowledge of how to treat? What if it comprised up to eighty percent of all known cases, was potentially fatal, and sometimes developed into other illnesses? What if doctors, because of their inability to diagnose this condition, took it less seriously than the more readily recognized forms of eating disorders—even though it was potentially just as deadly?

Such is the case with a disorder known as EDNOS, or Eating Disorder Not Otherwise Specified, a troublesome diagnosis that reflects larger issues in the mental health field. Practitioners are facing a situation in which they have no effective definitions for eating disorders and other psychiatric conditions that they are called upon to treat. EDNOS is so poorly defined that doctors frequently overlook it entirely, even though it is far more common than anorexia or bulimia, the better known forms of the disease. As a result, EDNOS sufferers often do not seek help until they have developed obvious medical complications and their disorders have grown significantly more severe.
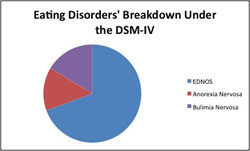
From units taught in health class and from our voyeuristic window into the personal struggles of celebrities and athletes, the American public is widely familiar with anorexia nervosa and bulimia nervosa, the two "full-syndrome" conditions in the eating disorders category. They both involve extreme symptoms and are easily recognizable for doctors and in society at large. EDNOS, however, functions below that level of public awareness. It is a catchall category, encompassing literally every other disordered eating pattern that doctors deem to be "of clinical significance," from binge eaters who do not purge, to purgers who do not binge, to starving daytime dieters who overeat at night. EDNOS also applies to "mild" cases of the other two disorders. It is the category for a subclinical anorexic who has every symptom of full anorexia except one or two; it's the diagnosis for a subclinical bulimic who purges once a week instead of three times. The category is so vast and unspecific that researchers and patients have a hard time understanding what it includes, and what constitutes "clinical significance."
The problems with the treatment and diagnosis of EDNOS stem from its non-definition in the DSM, or the Diagnostic and Statistical Manual of Mental Disorders. This is a volume that standardizes the classification of diseases for the mental health profession, and that has not been updated since 1994. The DSM vaguely defines EDNOS as any seriously disordered eating pattern other than anorexia or bulimia—an ambiguous non-description that tells doctors neither what the disorder is nor what it could entail. There is, however, a good chance that this confusion will change in the next two years, as a team of experts is working on the manual's next edition for a 2013 release.

Click to enlarge
Photo courtesy of Courtney Emery, via flickr
Meanwhile, clinicians who treat eating disorders complain about the flawed system established in the current DSM, known as the DSM-IV. As one such clinician, Alyssa Mandel, put it, "You cannot compartmentalize mental illness. It's too broad." The Arizona-based therapist specializes in treating eating disorder patients at a Scottsdale center that she founded and runs. "Easy access to information about eating disorders in the diagnostic form is what DSM-IV is supposed to be. And we don't have that," she said. "And that's what we need."
The way the manual defines an illness informs the work of the entire mental health field, including doctors, clinicians, researchers, hospitals, health insurance companies, policymakers, pharmaceutical firms and advocacy groups. All of these stakeholders rely on it to classify and help in the treatment of the nearly fifty-eight million mental health patients across the United States. Because the DSM-IV's definition of EDNOS is so useless, critics say it frequently hinders treatment and has little practical application. Distinguishing the poorly defined disorder from anorexia and bulimia can also be hazy and controversial; and many clinicians believe those better-known categories, too, need better clarification.
The doctors now working on the manual's revisions are testing out various ways of addressing the issues that clinicians have raised, including plans to relax the stringent definitions of anorexia and bulimia and to establish other new eating disorder categories. Potentially, these measures could reduce the scope of EDNOS, which is considered too wide. The catchall category is likely to remain, however, under the unfortunate new moniker of FECNEC, short for Feeding or Eating Conditions Not Elsewhere Classified. Yikes.
The more general debate about the DSM in many ways mirrors the ideological split in Congress over President Obama's health care legislation. On one side are those who think the new DSM should be geared towards researching diseases even if it means clinicians can't treat patients as efficiently; and on the other are those who believe that the DSM should make treating patients the priority so that it helps sufferers qualify more easily for insurance coverage and treatment options. At this juncture, one thing is clear: if the psychiatrists who are revising the DSM do not fix the definition of EDNOS, it will continue to compromise the health of millions of patients.

Imagine how complicated a diagnosis of EDNOS must be for patients who have never heard of it, particularly when their doctors don't understand it, either. One former patient, who gave her name as Jamie only, agreed to meet with me at a Manhattan Starbucks one damp and chilly day last fall to recount her experience with the disorder, and to discuss the new DSM. As a senior in high school, she dropped nearly forty pounds, her weight landing below the healthy range but just above the cutoff point for anorexia. Her doctor recognized that she had some sort of eating disorder, and because she was out of the weight range for anorexia, he diagnosed her with EDNOS. Neither of them understood the condition well enough to be sufficiently concerned to prescribe a treatment plan. She decided to take matters into her own hands and lost two more pounds, making her a bonafide anorexic. "I wasn't a completely emaciated anorexic, but I had the mentality and all the other symptoms," she said. "And nobody was like, 'Oh my God' until I had the diagnosis. It was like, one pound, and then all of a sudden they were like, 'Oh my God oh my God, oh my God. You're going to go to inpatient.' But before, it was like, 'You're fine, you're fine.'"
At an average build and slightly above average height, she arrived for our meeting bundled up in an immaculately neat coat over a fitted black top, her sleek deep brown hair appearing effortlessly groomed. She sat up straight and seemed composed, her low voice animated as she relived her experience. Her pale eyes seemed to take deeper color as she explained her decision to lose more weight after the doctor's initial diagnosis. "I think in a way I did it on purpose," she said. "Because I was like, 'You're not taking me seriously.' I was the one who reached out for help, not my parents, not my friends, not anybody.... I was the one who was like, 'Okay, this is a problem.'"
How much a person weighs divides the camps between those who qualify as anorexic and those who are relegated to EDNOS. These lines between "subclinical" and full-blown cases are meant to clarify any ambiguity about which diagnosis an individual should receive, but they also create difficulties for clinicians. Many practitioners believe that psychological factors are more important than a patient's weight in determining the severity of an eating disorder. Psychological definitions, however, tend to be far less concrete; and insurance companies want the most objective criteria possible to determine whether a patient deserves coverage.
Tessa Addison is a licensed clinical therapist in Greenwich Village, whom I met at her office near Washington Square Park to discuss her complaints with the DSM-IV's definitions of EDNOS and the other disorders. Addison was the first to express a sentiment echoed by all two dozen of the clinicians I interviewed: that weight alone does not determine how sick a patient is.
"I was treating someone recently who had been in the hospital, diagnosed with anorexia, meeting all the criteria," she told me. "By the time she got to me, she had gained enough weight to no longer meet the criteria. She was not better. She was psychologically struggling just as much as she had when she entered the hospital."
Addison's comments could easily have applied to another patient, Emily Bell, a twenty-year-old college student from Dallas who has lived on the thin line between anorexia and EDNOS for the past three years. Bell met me for dinner to tell me about her experience with eating disorders, and said that she still struggles with them today even though she technically no longer qualifies as anorexic. "My parents thought, and I thought, that me eating a lot, and me eating all the time or whatever was recovery and I was better," Bell said. "But in reality, it was the complete opposite." Her disorder has simply taken the lesser-recognized form of EDNOS. "I'm going to eat this, I swear," she added as if in testament, glancing at the untouched chicken Caesar salad, dressing on the side, in front of her.
Addison explained the issue for clinicians like herself who use research-oriented definitions for these diseases. "For research purposes it's really important to differentiate diagnoses so that you can sort of compare and contrast," said said. "But I find clinically that it's not that helpful for me to distinguish, for example, between someone who has all of the criteria of bulimia and someone who has all but one or two of them... I would treat them exactly the same way."
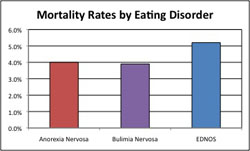
This is because patients who present with EDNOS and those who have full-syndrome disorders are, in many cases, equally sick. Recent studies by the nation's leading eating disorder researchers have found that many subclinical cases of anorexia and bulimia, which technically qualify as EDNOS, are in fact as severe as their full-blown counterparts. Additional research studies show that EDNOS can be as perilous as anorexia or bulimia. One such study on eating disorder-related fatalities found that EDNOS patients had a mortality rate of just over five percent, which is roughly one point higher than the rates it found for anorexics and bulimics. Patients across all three categories also shared a heightened risk of suicide.
Doctors may be arguing still over how and where to set the line between subclinical and full disorders, but most professionals by now agree that the current threshold is wrong. William Walters, who works as an administrator at an eating disorder advocacy group, summed up the problem in two sentences: "Research is clear that EDNOS is serious and life-threatening... It's an undefined catchall category of widely varying disorders that, even as serious and life-threatening as they are, don't get the serious attention they deserve."
The issue is not lost on patients. One told me that the change to the label of her diagnosis did not reflect an increase in her disorder's severity. It was her state of mind, not her dwindling body weight, she believes, that dictated the seriousness of her condition. "It's completely about mentality, which is why I have a problem with the diagnosis anorexia, why I have a problem with a lot of these diagnoses," she said, confidentially lowering her voice. "Because it's your mind... I don't think it should matter what the weight is."
For a disorder that is so poorly acknowledged and understood, EDNOS is quite prevalent, creating a further burden on clinicians. What was meant to be a residual category makes up at least sixty percent of all eating disorder diagnoses. Dr. James Greenblatt, an administrator at Walden Behavioral Care center, told me that EDNOS patients comprise close to eighty percent of those treated at the Massachusetts facility. What was intended to be a minority diagnosis is now the dominant category, which is especially troubling in light of the lack of public awareness surrounding it.
Many clinicians say that this goes back to the DSM-IV and its unhelpful classifications for all three eating disorder categories. These practitioners argue that EDNOS cases with the characteristics of anorexia and bulimia should be reclassified as full-syndrome. In addition, EDNOS cases can serve as a way station between anorexia or bulimia and complete health, a midway point that patients pass through as they move from disease to recovery. Overwhelmingly, doctors agree that these conditions are messy and do not fit into the neat, narrow definitions provided in the DSM-IV.
"Most clinicians are seeing patients who are binging, purging, then dieting, then cutting, then using drugs, then doing other stuff—a little bit of everything," said Dr. Douglas Bunnell, who directs outpatient services at the Connecticut branch of eating disorder treatment facility the Renfrew Center. "That's sort of their normal patient," he said. "But the research literature continues to talk about pure anorexics and pure bulimics." Sometimes, he said, what comes down from researchers as definitive guidelines "doesn't really connect up well with the clinical reality and the messiness of what we're seeing at our offices."
The frustration Bunnell expressed is also about the pervasive power of labels. Not only does a diagnosis of EDNOS marginalize a patient with insurance companies and treatment specialists but it also creates its own stigma among patients, where an eating disorder hierarchy has emerged with anorexia at the top. Within the community of sufferers, EDNOS is taken less seriously than its full-syndrome counterparts.
Insurance companies are notoriously strict about providing coverage for mental disorders in general and for eating disorders in particular. Although some states are adopting measures called "parity laws" that would mandate coverage for patients with mental illnesses, many insurance companies still fail to provide adequate support for those with eating disorders. The problem is not new. The media has publicized the issue, filmmakers have documented it, and doctors openly acknowledge the difficulties patients face in getting coverage for intensive treatment. Insurance companies generally do provide some level of coverage for anorexia and bulimia—though not enough, clinicians say—particularly in states that have adopted these parity laws. Such, however, is not the case for EDNOS.
This puts doctors, not to mention patients, in an unfortunate position. Two patients can be equally sick mentally but if one is EDNOS and the other is full-syndrome, they will receive different levels of coverage. Clinicians face the ethical dilemma of whether to give EDNOS sufferers a technically correct diagnosis as defined by the DSM-IV and the health insurance system, or to skew the diagnosis so that patients will qualify for insurance to cover the care they need. "It's a problem for clinicians," Addison said. "You don't want to commit insurance fraud, you want to give the appropriate and correct diagnosis. But you also want your patient to get coverage, because you know they're sick and they need the help."
Click to enlarge
The patient I met at the Starbucks elaborated on this idea, citing her personal experiences. "Sometimes you need that diagnosis of anorexia to get the insurance coverage, to get the validation that you have a medical issue, to be covered," she said thoughtfully, explaining that she probably would have never received help had she not dropped the two final pounds. "So in some ways, it's better to be worse. It's better to be sicker. Otherwise, you're not going to get help.... And in my situation, that's exactly what happened."
Sheri Rosenfeld, a therapist based in Washington, D.C., recounted the story of a patient whom she did not treat, a young woman who suffered from anorexia before developing a habit of binging uncontrollably several times each week. The patient eventually checked herself into a treatment facility, her case having progressed to the point that she was dangerously close to a nervous breakdown. Rosenfeld said that after a lengthy process of elimination, doctors finally gave the young woman a diagnosis of EDNOS, which was not covered by her family's health insurance plan.
"So that [EDNOS] is what she had," Rosenfeld said. "And the insurance refused to pay. So they paid twenty thousand dollars in one day, out of pocket, because she was unsafe. She really was... She wasn't going to kill herself, but she was harming herself."
The family appealed the insurance company's decision three times, to no avail. Rosenfeld described also how the doctors who saw this patient had little knowledge of how to treat EDNOS, adding to the young woman's confusion at receiving a diagnosis she had never heard of before. This is not uncommon: psychiatrists and hospitals tend to rely at least in part on a diagnosis to understand a patient's case, and the lack of understanding surrounding EDNOS confuses them.
"Even really good doctors that [the young woman] went to... and this is a very prominent university hospital—they just didn't understand what to do with it," Rosenfeld said. "It feels very black and white. I think people have wrapped themselves around anorexia and bulimia... it can be crazy-making."
Dr. Greenblatt explained that the families of EDNOS patients can feel overwhelmed and frustrated by the mixed messages from treatment professionals. If an individual is diagnosed with diabetes or a certain kind of cancer, he explained, practitioners will respond using thoroughly researched and approved treatment protocols. If a patient is diagnosed with EDNOS, however, a dozen different clinicians may recommend a dozen different treatment programs, with no real understanding of which option is best. This misunderstanding, he said, confuses patients and their families and can ultimately undermine their trust in the doctors who are trying to treat the patients, or lead to doubts that the illnesses can be treated at all.
When designing a treatment plan, therapists and psychologists pay less attention to a patient's diagnosis than psychiatrists do. These experts too, however, find themselves compromised by the lack of knowledge about EDNOS. They are better-equipped to handle the full-syndrome disorders, and for that reason, they tend to pay more attention to them.
Dr. Bunnell reflected further on the hierarchy among eating disorder patients, especially as it occurs at residential treatment centers. In a community of naturally competitive people who are all working to be the thinnest, anorexia is the equivalent of the Holy Grail—the standard that others perversely struggle to attain. As one clinician quipped, "The disorder that makes your body the thinnest is the best disorder to have." Which affliction occupies the next level down is not entirely clear, but clinicians and recovered patients said that bulimics were next in line followed by binge eaters, who are technically EDNOS. The other EDNOS patients seem to be distributed individually based on their cases and symptoms.
The patient I first met at Starbucks first described the hierarchy to me. "That's kind of what happened with me," she said, reeling out the story in a way that seemed almost protective of the disorder that had once made her feel special. "The ultimate goal was to be anorexic and have that control. And I got there, and it was so powerful, I felt so powerful."
Bell drifted into a similar rapture when recalling her bout with clinical anorexia. She saw a therapist and a nutritionist during her junior year of high school, but her disorder didn't improve. "Nothing changed," she said. She simply told the nutritionist that she was eating more. "I liked what I was doing, and I liked the attention from losing weight. I got so much attention. I started modeling." Losing herself momentarily, she added, "Junior year was a great year."
A patient of Dr. Bunnell's summed it up more flippantly. "We were in a group discussing this sort of issue," he said, "and one patient said, I think it was, 'Anorexia is like Saks, and bulimia is Target, and binge eating disorder is Wal-Mart.'"
Some clinicians speculate that the fixation on anorexia is a twisted extension of cultural ideas about thinness and beauty. Women's fitness magazines crowd newsstands, promising easy diets; slimmer, "better" bodies; new selves. Natalie Portman fought her way down to a clinically anorexic weight for Black Swan, only to have her punishing diet and workout strategies marketed to the public as an acceptable weight loss plan. Eating disorder victims may be so terrified of becoming overweight that they forget that the other, the underweight, side of the spectrum is dangerous, too. These patients may simply be buying into normal cultural ideals, but taking them too far. Deborah Klinger, a therapist who treats eating disorder patients at her private practice in Chapel Hill, North Carolina, said that she doesn't believe that our culture causes eating disorders but it does act like "a petri dish, just the right environment for eating disorders to grow and flourish."
The issues with the DSM-IV's categories of eating disorders do not necessarily reflect ineptitude on the part of their creators. The manual has been a rope in a tug-of-war by the same groups who are currently fighting over the revision process. The question now, clinicians told me, is whether the DSM is capable of appeasing both researchers and treatment practitioners, or whether it is inevitably fated to favor the needs of one side or the other.
Psychiatrists originally developed the DSM to provide a standard definition and categorization system for mental disorders in the United States, primarily for research purposes. Doctors revise it periodically, updating the system to reflect changing social attitudes and scientific discoveries. It not only influences the work of researchers and clinicians, it dictates it. The fifth iteration of the manual will be the DSM-5—the Arabic numeral will replace the Roman—and doctors are in the process of putting it together for its release in two years. It will be the psychiatric bible's first overhaul in nearly two decades, and a task force of experts at the American Psychiatric Association is in charge of its development. The team's top priority is to make the manual more accessible and helpful for clinicians in treating patients, but it is unclear as of now how far they will be able to go.
The American Psychiatric Association published the manual's first edition in 1952, a version that now seems wholly out of date with its description of homosexuality as a mental illness. This definition remained on the books until the DSM-III, published in 1980, which was also the first edition to establish eating disorders as an independent diagnostic category. The DSM-IV is the first to identify EDNOS as an official diagnosis. An appendix at the end of DSM-IV notes that binge eating disorder may warrant classification as a separate affliction in future editions, but that more in-depth research would be needed first.
Ultimately, the DSM attempts to convert the hazy, nebulous realm of the psychological into standardized, concrete definitions of disorders that warrant medical treatment. This process is bound to be difficult: it is necessary in order for doctors to recognize, research, and treat mental disorders on the same scale they do medical illnesses, but the subjective nature of psychology makes it difficult for doctors to flesh out definitions of illnesses that everyone can accept.
Even the doctors who lead the revision process have expressed misgivings about the system. Robert Spitzer was one of the most influential psychiatrists of the twentieth century, and he helped design the modern classification system for mental illness through his work revising the DSM-II to create the DSM-III. This edition took a new approach to diagnosis, introduced new categories of mental illness, and was credited with sparking a revolution in the field of psychology as doctors around the globe began to adopt it and use it to treat patients.
This version transformed the mental disorder classification system. Instead of placing socially driven judgments on diagnoses and broadly defining archetypes of diseases, the psychiatric community began to treat symptom-based, homogeneous categories of disorders. Spitzer chaired the team that led this transformation and was given credit for improving the standing of psychiatry as a medical field. Years later, however, Spitzer expressed some regret about his creation. In a 2007 interview, he told British documentarian Adam Curtis that the new approach to psychiatry may have caused a massive over-diagnosis of mental illness, and estimated that twenty to forty percent of the currently diagnosed population may be needlessly treated under the system.
The difficulty that doctors face when they attempt to approach and define mental illness using objective criteria compounds another problem. Doctors originally developed the DSM for research purposes, and the DSM-III's paradigm shift to a more science-based approach reflected an attempt to clearly and objectively define these difficult diagnostic categories. Doctors sought to create reliable and concrete definitions of illnesses even if they were unsure about the disorders' validity; and some experts argue that in their arbitrariness, these doctors may have been overly conservative in where they established defining lines between diagnostic categories. The team of psychiatrists charged with revising the eating disorder definitions for the next DSM are working to reestablish these lines in places that clinicians may find more useful, but say they are still placing a premium on categories that are rigidly defined.
Dr. Jennifer Thomas is a psychologist and the author of several prominent studies on EDNOS and other eating disorders. "Right around the DSM-III and DSM-IV there was a big movement to incorporate, as much as possible, science into the diagnostic categories," she said. "And because we didn't know a lot about the validity of the categories, people really focused a lot on reliability. So what that means is that they wanted people to confer the same diagnosis in Boston as another diagnosing clinician would confer in New York or in Hong Kong. And so they tried to make the criteria be really specific."
"But the problem is," she added, "they didn't know actually how valid those cutoffs [between EDNOS and other disorders] were, or whether it really mattered whether you were binging twice a week or once per week, they were just focusing more on whether you could actually make the diagnosis."
Although invalid cutoffs can result in faulty research and undiagnosed patients, the DSM's controversy extends beyond the placement of dividing lines. Robert Spitzer's comment about "over-medicalization" speaks to a growing concern within the mental health community, and a fear that the public may be over-diagnosed and over-medicated. The DSM has also garnered criticism from skeptics who believe that the manual's development is too influenced by politics, and that the final product is compromised as a result. Even the doctors who create it acknowledge the role that politics plays: in 2005, Spitzer spoke with two doctors who wanted controversial categories of sexuality disorders removed from the DSM. Spitzer acknowledged that the definitions of these disorders were flawed, but said that certain diagnoses would remain in the manual because their removal would result in "a public relations disaster for psychiatry."
The definition of EDNOS within the classifcation of eating disorders is a microcosm of the DSM's issues, especially in the way it highlights the disparity between scientific theory and clinical reality. "I think the fact that as medical professionals we can even come up with a term EDNOS for the majority of patients that are suffering reflects to me how little we know about how to treat eating disorders," said Dr. Greenblatt.
One huge problem that the DSM revision team faces in making a clearer definition of EDNOS is the variance in characteristics and behaviors that currently fall under this category. The other disorders are homogeneous: anorexics all share certain psychological characteristics, as do bulimics. The same is not true of EDNOS—binge eating disorder is drastically different from night eating syndrome, and both are completely unlike subclinical anorexia.
The narrow definitions of anorexia and bulimia speak to researchers' need for "pure" categories of eating disorders, applying only to the sickest of the sick. The DSM's definitions for these categories may not be useful in clinicians' efforts to treat patients, but they do serve experts who study the disorders. One group must work with definitions that are flawed or useless for its purposes so that the other group may excel. The doctors working on the current version contend that this is not necessarily true, that the document can serve clinicians and patients while still helping researchers, too.
Clinicians, however, say that they still need a more practical, reality-based classification system for diagnosing eating disorders. "These are man-made diagnoses," said Alyssa Mandel, whose treatment facility sees a wide variety of eating disorder patients. "And human beings are not that black and white. They're complicated."
Click to enlarge
"That's a human man-made creation, the DSM-IV, 5, whatever you want to call it," she added. "And humans are not that simple. So it's a lovely idea, it's wonderful in many ways, because it does enable us to have some direction when we're treating people. However, it cannot be the end-all, be-all. We need to be a lot more flexible and give ourselves permission to not just go by a book."
Mandel is among those who argue that the strict criteria for anorexia and bulimia should be relaxed for the DSM-5 so that subclinical cases may qualify for full diagnoses, thus receiving insurance coverage and treatment options; and doctors are proposing to do just that. However, this puts researchers at the risk of studying populations that may prove too heterogeneous, undermining the efforts that help clinicians understand and treat these illnesses. The debate about the DSM revolves around not only where to draw defining lines between disorders, but also how they should be drawn. The DSM-5 team's effort to strike a balance between the approaches will determine the future of EDNOS, as well as other problematic diagnostic categories of mental disorders.
"Several principles were established to guide the DSM-5 revision process," reads the DSM-5 website. "The highest priority is 'clinical utility' � that is, making the manual useful to clinicians diagnosing and treating people with mental disorders."
The team of doctors working on the DSM-5 is broken down into "work groups" for the different categories of psychiatric disorders. These task forces then propose what changes should be made, and the American Psychiatric Association conducts field tests to determine which proposals will make the cut.
Predictably, this process is fraught with controversy, particularly because developers face the heavy task of closing the gap between conflicting needs and ideologies. Those who want the DSM to be geared toward researchers argue in favor of specific and stringent definitions; those who want it to be more treatment-oriented feel that the definitions should be more lax, allowing clinicians more freedom in diagnosing patients.
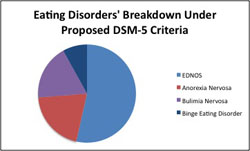
The task force has proposed, among other measures, relaxed definitions of anorexia and bulimia that would expand these categories to include many "subclinical" cases that are now considered EDNOS. Under the new guidelines, a woman would not have to lose her period in order to qualify for a diagnosis of anorexia nervosa, nor would there be a specific weight cutoff to differentiate anorexics from EDNOS patients. Likewise, patients who binge and purge would only have to do so an average of once a week to qualify for a diagnosis of bulimia, down from the stricter DSM-IV standard of twice a week. This would, theoretically, reduce the EDNOS category and allow cases that currently are considered subclinical to qualify for insurance coverage.
Dr. Anne Becker is a prominent member of the DSM-5 Eating Disorders work group who spoke to me in a telephone interview from her office at Harvard Medical School, where she is vice chair of the Department of Global Health and Social Medicine. She noted that some of the problems with the current DSM may lie in clinicians' interpretation of the manual. The controversial weight percentage cutoff point for anorexia, she said, is not actually a firm dividing line at all. The doctors who developed the DSM-IV included it as an example, and clinicians who misinterpret the number as a hard cutoff have since institutionalized it as such.
"In the DSM-IV there's an example of what a low weight would be, and that's been taken as really a concrete cut point by some people," said Dr. Becker. "It's most definitely intended as an example." She added, "That's why it says, 'e.g.', not 'i.e.'" Evidently, doctors have been misreading the "for example" as "that is" for nearly two decades.
The team has also proposed that binge eating disorder, which doctors have researched as an independent entity, be extracted from EDNOS and established as its own diagnosis. Researchers estimate that binge eaters account for a large percentage of EDNOS patients, so this change may significantly slim down the problematic category further. The proposed revisions note that within the renamed category FECNEC, several conditions—specifically purging disorder, night eating syndrome, and sub-threshold anorexia, bulimia, and binge eating disorder—may warrant their own diagnoses, but need further study before they can be established as such.
"By all means, we want to get the word out, because we hope that clinicians will be recognizing these profiles and observing how they do and generating hypotheses that then can be taken up into the design of clinical trials and will amass a database that will either say, 'Yes this is different' or 'No it's not different,'" said Dr. Becker. "This is all about understanding how the variation across individuals is patterned."
The further proposed changes to the eating disorder classification system would result in a broader definition of the term "eating disorder" to include cases in which patients have strange behaviors with food that are not driven by body image. For instance, the DSM-5 eating disorders task force has suggested the reclassification of a trio of diagnoses that formerly appeared in a category called "Disorders Usually First Diagnosed in Infancy, Childhood, or Adolescence." These include pica, a rare disorder in which patients crave such non-food items as clay, dirt, paper, and chalk; rumination disorder, in which a person repeatedly regurgitates food and then swallows it again; and ARFID, or Avoidant/Restrictive Food Intake Disorder. This applies to people who have aversions to food or eating for reasons unrelated to body image.
"It's sort of like—do you want to arrange your closet by color or by function, what's the best way for you to find things?" said Dr. Becker. "Obviously when thinking about the DSM, one of the questions would be do you want to organize disorders by the onset stage of life, or would it be better to organize like disorders with like disorders?"
"The intention is certainly not to reframe," she added. "I hope we'll get feedback from people who strenuously disagree or agree."
Klinger joined other mental health professionals in expressing mixed feelings about these proposed changes. Research clearly supports the idea that subclinical cases can be as serious as full-blown ones and should be reclassified; and clinicians almost universally support the proposal that the two full-syndrome categories be relaxed. "It's this process of refinement with greater awareness of different manifestations of disordered eating," she said of the DSM revision process. "The criteria for anorexia and bulimia are broader, the recognition that binge eating disorder is its own diagnosis is an important step, the addition of purging disorder to EDNOS... It's a process." Many, however, are skeptical that these proposed changes would be enough to substantially reduce EDNOS.
Dr. Thomas, whose studies informed the team's work, said that she was uncertain whether the proposed changes would actually narrow EDNOS in practice the way they do in theory. She said that research suggests that even if the full-syndrome categories are relaxed, there will still be "a substantial group that's left over having EDNOS."
Few major studies have explored the actual effects these changes would have. Clinicians are also uncertain about how insurance companies will react.
Addison laughed. "They won't like it at all," she said. "But I don't know they'll be able to do anything about it. Because I think, if it's in the DSM-IV, it represents the clinical consensus and the research has been done."
Others are more skeptical. While insurance companies generally use the DSM to inform their coverage of mental health, they are not bound to do so. "Not to attribute nefarious intentions to them, but it's possible that they could then add other criteria that somebody has to meet that aren't based on the DSM," said Dr. Thomas. "I'm not sure. I think it's too magical to think that just by changing the DSM, we can get everyone the care that they need."
Dr. Becker, however, defended the less popular idea that the DSM is not responsible for ensuring that patients who deserve care receive insurance coverage. "We can't make criteria to respond in sort of a chess match with insurance companies," she said. "Because that's really the tail wagging the dog. We can't sort of guess: what will move an insurance company to feel something is worth coverage? Partly because what the insurance company decides to cover is going to be driven by their financial bottom line, and it's ultimately socially constructed."
By and large, clinicians seem to approve of the DSM-5's attempt to recognize EDNOS subgroups as possible topics of further study. The DSM-IV noted binge eating disorder the same way in its appendix, which motivated doctors to research it and ultimately establish it as its own diagnosis. Therapists and psychologists say they see some of these subgroups in practice, but acknowledge that the behaviors aren't yet researched enough to warrant separate categories.
"I've got to give credit to the people that put [the] DSM together," said Dr. Steven Karp, who is the medical director at an eating disorder treatment facility in Austin, Texas. Dr. Karp expressed disappointment that purging disorder was not established as an independent diagnosis, but rather named as a residual category subgroup that warranted further study. "They don't do it willy-nilly, they want to see significant research that makes it unequivocal that it deserves its own diagnostic category. At this point, the scientists that look at it say, 'Yeah, it's an entity, but we need more research to make sure that it's a stable form of a disorder.'"
The responsibility for this task, however, may not lie with the DSM-5 development team alone. Dr. Becker noted the value in collaboration between clinicians and researchers, a sentiment I heard numerous practitioners reiterate. If the field is to close the gap between research and treatment, professionals may need to work more closely to produce reliable diagnoses that still reflect clinical reality.
"I think the pressure's on us as a field, researchers and clinicians alike, to come up with improved categories to describe the suffering that goes along with eating disorders," said Dr. Bunnell. "Clearly having anorexia, bulimia, binge eating disorder—doesn't really capture, unfortunately, for a lot of patients what's really happening with them."
Click to enlarge
Unfortunately, eating disorder researchers have limited capabilities. Eating disorder research is notoriously underfunded compared to other mental problems, despite the illnesses' high mortality rate. Eating disorder research currently receives twenty-eight million dollars a year in federal funding—a quarter of the funding provided for ADHD research, and less than one-tenth of that for schizophrenia. As a relatively new type of recognized mental illness, it has few advocacy groups helping it to secure funding in the way that, for example, schizophrenia and autism do. Dr. Karp summed it up succinctly: "We need more money in order to understand it and narrow it down, basically."
Meanwhile, clinicians and patients have other ideas about how to ensure proper recognition for people who will still fall into the residual category. One patient said she believes that the field should focus on early action for people who may be developing these illnesses, and said she hopes to one day create an intervention program for body image and eating disorders. Similarly, some psychologists have articulated the belief that pediatricians should be better trained to recognize early signs and symptoms, especially since these disorders commonly develop during adolescence.
The DSM-5 seems to be a progressive step, but doctors and clinicians agree across the board that the manual is still a work in progress. "I think that the best thing that could happen is more research," said Dr. Karp. "There are really smart people that are putting the DSM together. We recognize its weaknesses. It's the best we've got right now, of what we do have. And the only way it gets better is for us to study the various disorders more extensively, more thoughtfully, and we'll get more precise in being able to make good, accurate diagnoses."
Ultimately, it appears that EDNOS—or FECNEC, as it may become—will have to stay on the books. "There will always be a need for some sort of residual category or some EDNOS-like category," Dr. Thomas sighed. "It just shouldn't be the diagnosis that the majority of people have."
Amanda can be contacted at

