


Victor Avon spent years turning food into solace, ballooning to well over two hundred pounds during high school. Bullied for his weight, his non-surfer clothes, and the way he talked, high school in Wall, New Jersey, meant three friendless years. "In my eyes, the food was causing me to be like this, causing all the pain," he said. "Yet I turned to it to relieve the pain."

By age twenty, he found a way to change his life. Not by discovering healthy eating habits or hiring a personal trainer, but by getting sick. Not cancer, as his classmates whispered after he lost a hundred and twenty pounds in six months, but anorexia, a disease that consumed him for the next six years. As a sophomore at Monmouth University, Avon, at just over six feet, weighed two hundred and ninety pounds—a hundred pounds more than the maximum recommended weight for his age and height. By the time he entered treatment in 2008, he had dropped just over half his body weight. The scale read one hundred and thirty-four pounds. "The body is just a symptom of what's going on in the head," Avon said.
For Avon, there was no gradual cutting back on food. Once he made the decision to change his body, he ate the same meal twice a day, every day: a chicken cutlet, broccoli, and an occasional slice of cheese. He continued this routine through college, getting on the scale four times a day – first thing in the morning, at noon, at five p.m., and again at nine p.m. If his weight had not decreased, he hopped on the treadmill, sometimes after each weigh-in. On most days, he estimates that he burned three to four times as many calories as he consumed. Even after college, every other weekday he would down half a protein bar for breakfast and then lift weights at the gym near his office building during lunch time. At his desk, he would eat chicken and broccoli. Once home, he said he would do a thousand push ups and a thousand sit ups. Dinner was chicken and broccoli again. On alternate days, he ran eight miles on the treadmill at five o'clock in the morning, ate half a protein bar and four peanuts, lifted weights, went to work, ate lunch, finished his workday, and arrived home to exercise some more. "Every night, I would actually pray that I wouldn't wake up the next morning," he said. "Without overtly taking a gun or slitting my wrists, I did everything to kill myself with the sickness."
Avon's story may sound unusual but it isn't. In a landmark study in 2007, researchers at the Harvard Medical School found that one in four anorexics and bulimics are male, as are forty percent of those diagnosed as binge eaters. Yet, the phenomenon receives little national attention, largely because of its invisibility. While in women the disease most often manifests physically in scary-looking concave abdomens, protruding spines, and twiggy limbs, in men, the same daily regimen of intense exercise and severe restriction of calories helps achieve a desirably trim, V-shaped physique. In men, with fewer outward signs of the condition, it can go unnoticed, leaving them to suffer in silence, crushed by feelings of shame and isolation.
So the similarity between male and female sufferers is less physical than it is psychological, evident in the difficult relationships both have with food, exercise, and body image. The genders also respond to their illnesses differently. Women tend to come forward and admit to their disease en masse—for example, large numbers of women confessed to battling bulimia in the early 1980s—but men tend to come forward more reluctantly. At least that has been the pattern in the past fifteen years.
As the prevalence of eating disorders in men has come to wider attention, pop-psych books have appeared in the market, notably Making Weight: Healing Men's Conflicts with Food, Weight and Shape in 1999, and The Adonis Complex: The Secret Crisis of Male Body Obsession in 2000. While sufferers and their families found comfort in the publication of these books, they had little wider impact.
Leigh Cohn is one of the co-authors of Making Weight, and the president of Gurze Books, a publishing company that specializes in literature related to eating disorders. Not much has changed since his book was published, he said, except for more acknowledgement from clinicians that men do get eating disorders. "Ten years ago, if I were to ask a room full of therapists, 'how many of you have treated males,' there'd be just a few hands raised," Cohn said. "Now, if I ask the same question, most of the hands will be raised."
Among the experts, opinion varies as to whether there actually are more men suffering from eating disorders than in the past or if more of them are simply submitting to treatment. The latter is statistically supported: In 2006, the Healthcare Cost and Utilization Project found that hospitalizations among males with eating disorders increased thirty-seven percent from the period studied in 1999-2000 to 2005-2006. Specialists interviewed for this article attribute the increase to both situations—more men suffering and more admitting to the disease.
"The masculine ideal is very different than it was thirty years ago," explained Tom Hildebrandt, director of the Eating and Weight Disorders Program at Mount Sinai Hospital in New York. "As you see that, you're going to see more and more behaviors, like men who have a vulnerability, like they're really perfectionistic," he said. "When told, 'You have to look this way,' they apply this perfectionism to the pursuit of being a man, and substitute in excessive control of diet and over-exercise. Those things fit in, and it looks a lot like an eating disorder."
Hildebrandt suggested that a new, perhaps impossible-to-achieve male body ideal is partially responsible for the rise in male eating disorders. Others agree. Roberto Olivardia, who co-authored The Adonis Complex, referred to a series of surveys that appeared in Psychology Today, also cited in his book. Between 1972 and 1997, the number of men who expressed dissatisfaction with their overall appearance jumped from fifteen percent to forty-three percent, an almost three-fold increase. Olivardia attributed the shift in part to the rise of Hollywood stars with chiseled physiques like Sylvester Stallone and Arnold Schwarzenegger.
Click to enlarge
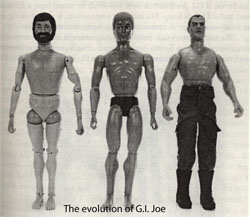
Even boys too young to have seen Schwarzenegger in The Terminator were playing with action figures. G.I. Joe, who had no abdominal muscles when the toy was first manufactured in 1963, first got some definition in 1975. By 1994, he had the muscles of a professional bodybuilder. The title of the 1999 study, "Evolving Ideals of Male Body Image," says it all.
This evolving male ideal mirrors the Barbie phenomenon. Boys as young as three years old are being presented with an impossible physical ideal for which to strive. "Marketers said, 'We now have the power to make men hate their bodies as much as we make women hate their bodies,'" Olivardia said, hearkening to the pattern of dots on a scatter graph in the book. While the proportion of undressed females in popular magazines such as Cosmopolitan and Glamour has remained fairly steady over the past twenty years, the proportion of undressed males has shot upwards. In the late 1950s, three percent of men in these magazines were naked or scantily clad. By the 1990s, the percentage had risen as high as thirty-five percent.
These are not the only cultural norms to shift over the past half century. The 1970s and 1980s were filled with feminist milestones—Roe v. Wade, the debut of Playgirl, the all-female Go-Go's hitting the top of the Billboard charts. During these years, more women entered the workforce and became financially independent, putting them in a better position to be selective about their mates. As Olivardia put it, women in this increased position of power could then say, "I want my guy to lose ten pounds." Other specialists take a different view. "It's hard for me to rectify how women voting turns into men wanting to starve themselves," Hildebrandt said. "There's no real, solid link."
Dr. Mark Warren is the medical director of the Cleveland Center for Eating Disorders, and while he accepts that the media and feminism can be triggers for the disease in males, he thinks the cause is primarily biological. If eighty percent of Americans go on a diet each year, and only five to six percent end up with eating disorders of any kind, it stands to reason, he said, that biology must be at least partially responsible.

So, who are the men developing eating disorders, and why? Avon, for instance, attributes his disease to years of being bullied. Kelly Stolberg, a clinical social worker at the hospital where Avon was treated, affirmed that bullying is a contributor. Of the men she has worked with at Princeton University's Medical Center, negative body-related comments from friends or love interests have often been an onset trigger. The idea is planted, and the plan to go on a diet spirals out of control—sometimes abetted by well-meaning relatives who encourage the weight-loss regimen. For example, the grandmother of Clayton Kammer, with whom he was living at the time, put her grandson on his first diet at age eleven. That sent him to the store to buy Little Debbie's Hostess cupcakes for binges with any money he could save up. By the age of thirteen, at his mother's house—always filled with the junk food she bought with food stamps—he figured out how to purge.
"Bingeing was kind of cool," he said, "because I had to put together in my own head that I could eat these large quantities of food, throw them up, and I wouldn't have to hurt over it. I wouldn't have to suffer." Over the years, he learned what foods he needed to regurgitate immediately and which – mushrooms, pineapples, and meat – he could force out later on.
At his heaviest weight of two hundred and sixty-eight pounds, he was twenty-one and five feet nine inches tall. By the time he sought treatment three years later, he was bingeing and purging as often as twelve times a day and had dropped to one hundred and thirty-nine pounds. But his hair was thinning and his body was aching. Kammer was in a state of "absolute depression, always had anxiety, could never catch my breath." Grocery trips several times a week would cost him up to four hundred dollars. "Really, the only thing I could do was binge and purge," he said. "I didn't have time to do anything else."
Ron Saxen knows firsthand what Kammer endured. Although Saxen never made himself vomit, he sometimes ate just as much. A nineteen-year-old model who suffered from binge eating disorder, he severely restricted calories and exercised in excess. Saxen described waking up in the morning, running five miles, drinking a cup of coffee and eating a banana, biking twenty miles, drinking a second cup of coffee, swimming thirty laps, and lifting weights. He then visited Skinny Heaven, a shop where he would indulge in a banana split with a calorie count of three hundred and thirty-five. By late afternoon, he had eaten four hundred and fifty calories and burned off thousands. "Eventually, I was always going to fail," said Saxen. But this was the 1980s, and Saxen knew nothing about eating disorders. "I figured I was totally insane. I was a party of one. I was uniquely flawed, and the answer was to be strong, buck up and get over it. It became a fight for the next ten years."
Saxen fled the New York modeling scene, embarrassed and unable to halt his bingeing. He stopped picking up his phone or calling his friends. He watched himself in a television commercial, and saw his face on the cover of a book titled Sports Fitness and Training. But, by the time those images became public, they no longer looked much like him. Saxen gained a quick fifty pounds, bingeing on ten thousand calories at a time without purging. "Think about an entire half gallon of ice cream," Saxen said. "Then, think about five king-size candy bars at eight hundred calories a bar. Five times eight is four thousand. The ice cream gets you to like six thousand calories. Hostess Fruit Pies, four or five of those. Those are four hundred calories each, so with that, you're at eight, nine, ten thousand calories. I would tell myself, 'Okay. This is the last binge I'm going to do. Tomorrow, I'm going to be perfect for the rest of my life.' I would just keep going and going until I absolutely physically could not put one more bite in my mouth because I knew that was the last party I was ever going to have."
But the party didn't stop. Throughout his twenties, Saxen worked in sales, a field that allowed him to keep irregular hours and work independently. If he had to be on a sales call at 6 a.m., he would wake up at 3:30 a.m. to run. Nonetheless, his weight swung eighty pounds up and down. Saxen eventually wore out his patella tendon, the muscle that connects the quadriceps to the tibia, until the left one became detached. Running was no longer an option.
Saxen's experience is far from unique, although he did not know it at the time. Dr. Warren of the Cleveland Center for Eating Disorders explained that binge eating and compensatory exercise is the most common form of eating disorders in men. "If a woman says, 'Last night, I went out and ate a giant pizza and then I ran for three hours,' you're thinking boy, there's an eating disorder here. On the other hand, if a guy says, 'I ate a whole pizza and then went running with my friends. I ran five miles,' he's unlikely to be sent for eating disorder evaluation." Because the disorder looks and sounds different in men, it is harder to spot.
There are also men like Troy Roness, a diagnosed anorexic, who engage in compulsive exercise without the binge. It is a curious combination. Exercise serves the same role as purging, a means of compensation. However, there are no ten thousand calories of junk food to work off. Roness claimed he never stepped onto a scale until he began exhibiting eating disorder behavior around age twenty. Weight was not his core issue, but part of a quest for perfection and control. "That number on the scale is, okay, did I succeed or did I fail?" Roness said. "It's about what's deeper."
As he exercised his way to a trimmer physique, friends and family lavished him with compliments. Flattered by the positive attention, he fell into a self-perpetuating cycle. As his fitness routine grew more intense, his food intake decreased to almost nothing. At his sickest, Roness ate lettuce, carrots, and yogurt once a day. He also added a fifteen to twenty percent incline to the treadmill, ran up to eight miles, lifted weights, and did abdominal work daily. His job as a gym teacher allowed him to remain active throughout the day. If he sat still, he would return home feeling guilty. "I was addicted to it," Roness explained. "Your body becomes accustomed to it. It craves it. It wants it. That was my drug at that point."
Roness couldn't stop. His skin became jaundiced. He tasted blood while running. But instead of giving himself a break, he swallowed painkillers. That way, he could wake up the next morning and keep going. The behavior had caused severe physical deterioration but he was too psychologically ill to stop what he was doing.
In retrospect, Roness might not have gotten so sick if his physician had recognized the signs of an eating disorder. Roness' mother, concerned that her son had cancer, sent him to see an internist. The doctor ran blood work, only to diagnose Roness with hypothyroidism. Slowed thyroid function is a common symptom of anorexia, and the medication she prescribed accelerated his already dangerous weight loss. An eating disorder was never suggested.
Roness never sought professional help for his anorexia until he was moved to make a desperate call to Dr. Phil's daytime talk show. Before Roness flew to a treatment center where he would receive help, he underwent a medical evaluation in order to be given the okay to fly. The physician who performed the exam found that both his kidneys and liver were shutting down and that if he didn't start eating and stop exercising, he would die within a month. Once in treatment, Roness learned he had suffered a small heart attack, likely while running or sleeping. If his first doctor had asked different questions, Roness might have gotten the help he needed sooner. "It's very disappointing to know that men who are struggling with eating disorders can go out and maybe try to reach out for help to somebody," he said, "that they don't want to say it, but maybe they want to be found out, and even those in the medical profession aren't working in that direction."
Although primary care physicians are not always the most astute at recognizing eating disorders in either gender, they are far more likely to connect a woman's symptoms to the illness. Doctors, like other Americans, are less culturally attuned to the idea that men can be as vulnerable to these conditions as women. "I've had many male patients, boys who have been anorexic and their physician might assume it's a gastrointestinal issue," Dr. Olivardia said in a recent telephone interview. "They don't even entertain it could be anorexia nervosa. When you have a doctor not even asking you if you're starving yourself, the message you get is, 'Oh my God, this is so out of the ordinary. It's so bad. It's so unthinkable.'" He recalled a recent case in which a boy was dieting towards emaciation, but whose doctor never asked the boy whether he was restricting his diet, or whether he had any body image issues or concerns. In the meantime, studies such as "Mortality in Anorexia Nervosa" published in the American Journal of Psychiatry, have found that eating disorders prematurely kill more Americans than any other mental illness. The rate of death from anorexia is two hundred times greater than that from suicide.
As doctors, parents, and friends fail to recognize this kind of suffering in the men in their lives, those afflicted with eating disorders tend to retreat further into their illnesses. "Every man I've ever treated with an eating disorder feels a sort of shame in terms of their masculinity," said Dr. Olivardia. "When you have anorexia, you are very fragile, and you're not very strong. Your voice is not loud. You're not assertive. Many of these men do have issues with assertiveness and confidence. Those issues get framed and are an assault on their gender identity in a way you don't see with women."
Ron Saxen turned his experiences with the disease into a book called The Good Eater: The True Story of One Man's Struggle with Binge Eating Disorder. But even after sharing his story with anyone who saunters into a Barnes and Noble or logs on to Amazon, he is ashamed. At a party shortly after the publication of his book, Saxen's proud wife bragged about her husband's accomplishment. He motioned for her to be quiet. "I don't want these guys to look at me like, 'What are you gay or something?'" Saxen said to me. "So, I'm thinking, they're thinking I'm gay, They don't want to get along with me. They're thinking I'm some kind of fucked up wussy weirdo. I just had to get her to stop."
Patrick Bergstrom, a recovered anorexic and a speaker and activist for the National Eating Disorders Association, known as NEDA, still confronts feelings of shame, partially attributable to a stereotype that he, like Saxen, is uncomfortable with. "Most people think that I'm a gay guy that had an eating disorder," Bergstrom explained. "That could be another reason that a lot of guys don't want to admit to it. It's seen as such a feminine thing. You're a weak guy because of it." Although studies conflict about whether eating disorders are more common among gay men, those researchers with whom I spoke attributed any increased prevalence to a different set of social stigma. Gay men may simply be more comfortable admitting to their illnesses. Of the ten former sufferers I spoke with, only two are gay.
As CEO and president of the national association, Lynn Grefe has seen how difficult it has been over the years for men to find treatment centers, and how the inability to get concerted help perpetuates the cycle of humiliation. "It made it tough for a guy to talk about it when there was nowhere to go and get help," she said. Grefe mentioned the program at Rogers Memorial Hospital in Oconomowoc, Wisconsin, a treatment facility that dedicates one of its three floors exclusively to men. Troy Roness received his treatment at Rogers during two separate eighty-one-day stints. Embarrassed to be a man with an eating disorder, Roness believes that being in a single-sex program was extremely beneficial. He found camaraderie with the other men in the unit and was comforted by hard evidence that he was not the only man having such experiences. Consequently, he found it increasingly easy to open up during both group and individual therapy sessions.
Avon was hesitant to enter treatment at Princeton University Medical Center in New Jersey, an inpatient program that accepts both males and females. Although he packed a bag, as instructed, for his initial evaluation, he assumed that he would be sent home. "I didn't think I would fit in," Avon recalled. "[I thought] If I come, they're going to think I don't belong here." He described his program as "ridiculously hard." Each day began at 6 a.m. with vital signs checks and continued with weigh-in, supervised meals and a variety of therapies – group therapy, psychotherapy, art therapy, and relaxation therapy. Avon, as the only male among twenty-three inpatients and ten outpatients, soon took on the role of big brother. "My mission was, I know this sucks, but we're all in this together," he said, adding that the challenges of being the sole male in treatment accelerated his own recovery.
While gender-segregated treatment may be more comfortable for males, there is no proof that men treated in this manner recover faster, more completely or more frequently than those who receive treatment in co-ed facilities. "You're treating the same disease whether it's a male or a female," said Dr. Olivardia. "You're treating anorexia. You're treating bulimia. There aren't two different types of anorexia, one for males and one for females." Perhaps the greatest advantage of male-only treatment is its potential to normalize eating disorders in men. If these centers received more publicity, more men might grasp how prevalent their conditions are.
Even with the growing number of resources focused on treatment, full recovery still may never be possible. Men in recovery may give up, or at least curtail their most extreme behaviors—starvation, bingeing and purging, and obsessive exercise. But, many believe that they have not, and never will fully leave their diseases behind.
Snowden Wright is a freelance writer with an MFA in fiction writing from Columbia University. Almost thirty years old, he has never lost the legacy of his early teenage anorexia. In fact, he wrote an essay about the experience that appeared on Slate just last December. Wright's anorexia whittled his weight down to seventy-six pounds. He believes an eating disorder is an addiction that a person never escapes. "When you're drinking or doing drugs, you know it isn't good for you, but something inside you keeps compelling you to do it," he said. "Same with this. Even when you're over it, it's still hanging there in the back of your mind. I don't think any alcoholic ever stops wanting to drink. In the same way, it'll always be there, itching, nipping at your heels."
Clayton Kammer, since returning home from treatment last May, still thinks of life in terms of opportunities to eat cake. He has given up bingeing and purging and haunting the junk food aisles several times a week, but still will say, "Today, I wouldn't say I'm comfortable having a birthday cake in my house. But, could I have a piece of birthday cake if I went somewhere? Absolutely. Would the thought to throw it up cross my mind? Probably once." Kammer allows himself to think about purging for a few seconds, and then forces the thought away.
Many of the men I spoke with said sharing their stories proved a therapeutic and essential part of their recovery processes. Kammer does not speak publicly, but he is open about the everyday struggles of life after eating disorder treatment. Those who call his cell phone are greeted with a ring-back tone – "Seasons of Love" from the long-running Broadway musical, "Rent." The song asks, "How do you measure, measure a year? In daylights, in sunsets. In midnights, in cups of coffee. In inches, in miles, in laughter, in strife." Kammer measures his days in time free from the grip of his eating disorder. One of his Facebook status reports reads, "Today was a difficult day, but one more day without ED," a common abbreviation of eating disorder within that community. "When people who are recovered or in recovery from bulimia know they can talk about it, just by talking about it, they're going to save lives," Kammer said.
Roness speaks about his experiences even more publicly. As a spokesperson for the national association, he shares his story on its website. He also maintains a blog on the website of This Emotional Life, a PBS series that focuses on mental health issues. While studying for his master's degree in education at Minot State University in North Dakota, Roness travels across the state to spread what he calls "the word of recovery." What began as an outlet for dealing with his own tangled emotions became a way to help others. "In North Dakota, there's a gravel road," Roness said. "I think about all the potholes and the rocks and everything that are in that. If I can go along on that journey and fill a couple of those in, so that the road isn't as rough as it would be or it could be, then that's all that matters." After a speech at the school where he once taught physical education, an eighth grade girl and former student approached Roness to tell him that he was her hero. While Roness had never thought of himself in such terms, he said that experiences such as that one keep him focused on getting, and staying healthy.
In the way that academic literature on male eating disorders flourished a decade ago, now is the moment for memoirs. I first met Victor Avon at the NEDA walk last October. Although I was told that there were many struggling men present, there were very few men standing at the exhibition booths. Large groups of women arrived, either in recognition of their own struggles, or to support friends and family members killed by eating disorders. Most of the men claimed to be walking for girlfriends, sisters, or daughters. But, Avon was promoting his book, My Monster Within: My Story. He wrote it because when he was gravely ill, he had trouble finding books about men with eating disorders. He came across My Life as a Male Anorexic by Michel Krasnow, which he deemed anti-recovery. Nonetheless, Avon competed with the author, whom he knew died one year after publishing the book. "It was like fine, you did all that and you died," Avon said. "You know what? I'm going to do all that and more, and I'm going to live. I'm going to beat you. I did beat him and I somehow lived. But, I did not want other people to only have that out there as their sole thing to read." Although My Monster Within is honest and thus at some points difficult to read, it concludes with a sense of hope.
Ron Saxen had a different experience in the bookstore. He wrote The Good Eater because he was so thankful for the material he found on the shelves. The Eating Disorder Source Book and Binge No More: Your Guide to Overcoming Disordered Eating proved to Saxen that after years of suffering alone, he had company. "If I had known sooner what I know later, it would have been a lot less years of suffering," Saxen said. "There need to be more people like me standing up and saying, 'Yeah, me too. Yeah, me too.' Because if there's enough me toos, we can get more people to come forward."
Or better yet, we can take preventative measures. Mark Warren, in addition to his job as medical director of the Cleveland Center for Eating Disorders, leads the Males and Eating Disorders special interest group for the Academy of Eating Disorders, a professional organization dedicated to leadership in the field. He suggested secondary prevention – conversations about food and body image for boys that are meant to identify the potential for disorders in elementary aged children.
Dr. Hildebrant of Mount Sinai agreed. Intervention is far more difficult when a man has been sick for years. "We're all passively accepting our culture," he explained. "The best intervention efforts for women have been asking them to act out against that, to act in an inconsistent way with those messages that you've accepted. It would be the same for guys."
But, Hildebrandt has a far more innovative idea. Men are much less likely to seek treatment for any health problem, mental or physical. "It's magnified tenfold in men with eating disorders because we don't have any novel or creative ways to break down those barriers at this point," he said. "Until we do that, we're probably going to be stuck with this misperception that men don't have these problems." The traditional model of psychotherapy where a patient sits in an office and talks about her feelings has not been successful in getting men into treatment.
Hildebrandt revealed an innovation with the potential to shatter this barrier: the use of technology to treat psychiatric diseases. For example, a self-help computer program would offer steps on how to overcome a binge-eating problem. The patient would log data, and an expert would sit on the other side of the computer. She would offer feedback and guidance, creating an experience that is personal, but also practical and accessible. Although there is no research of this sort in the eating disorder field, a group at Clark University in Massachusetts is currently studying a technological model for male-specific treatment of depression. If the researchers behind The Men's Coping Project fulfill their goal of better understanding men's well-being, they may be able to help men with eating disorders.
With such treatment programs years away, eating disorder advocates are focusing on legal mechanisms that would improve training for health care professionals, including a bill working its way through the New York State legislature. "Eating disorders are preventable and treatable," reads a memorandum about the bill on a state government website, "yet hundreds of people die from them each year. New York State must take the next step and pass this bill to ensure that our health care professionals are given the appropriate training and resources to adequately identify eating disorders and intervene so that these diseases are caught early and lives are saved." The legislation would require physicians, nurses, therapists, social workers, and dentists to complete an hour-long course in how to detect and treat the diseases.
In June 2010, both the senate and assembly versions of the bill were referred to their respective higher education committees. They remained there for the rest of the year only to be reintroduced in 2011, and as of early February, had returned to the committees. In the state senate, a notice of committee consideration was requested on April 4.
Assemblyman Peter Rivera, former Chair of the Assembly Committee on Mental Health, Mental Retardation and Developmental Disabilities, co-sponsored the bill. He said he has received no letters of dissent from the professional associations, although he does expect some complaints. "Whenever you have any issue of professional training, professional requirements or professionals changes, there's a tremendous cry that we encounter," he said.
Other legislators agree. Kathleen MacDonald, in her position as a policy assistant at the Eating Disorders Coalition, has experience with the obstacles that instructive bills such as this one can face. "People look at that as you're telling them what to do," she said. "A lot of people don't like that, even though it will save lives. Look at the seat belt laws. Look how long those took to pass. It gets really political."
There are also financial concerns. Rivera alluded to hesitation by the Office of the Professions to lobby for bills that would require hiring enforcement personnel to oversee the legislation's proper implementation. "There is a cost to all this stuff," Rivera said. "The question is, what is that cost? What is the cost to train? What is the cost to take the course? What is the cost to regulate it? These are the issues that aren't clearly addressed in the bill."
Assemblyman Felix Ortiz, the bill's co-sponsor, said he believes the financial obligation is worth assuming, even in a poor economic climate. "Sometimes, we have to pay now to integrate legislation that is going to have a positive impact on helping people," he said. "Prevention is the best measure to save money on health care and also to help people get health care."
Eating disorder advocates are watching closely. If New York passes the bill, it would be one of a small number of state legislative efforts on the topic to succeed. In 2005 in Texas, a mental health parity bill fizzled in its effort to force insurers to cover anorexia and bulimia as they do depression, obsessive compulsive disorder, and schizophrenia. In 2009, a Pennsylvania bill also failed. It would have required health insurance policies to provide coverage for treatment of eating disorders. Only twenty-three states include eating disorder treatment measures in their mental health parity legislation. In a country where less than half of states mandate that the diseases be covered by health insurance, prevention legislation would represent extraordinary progress.
NEDA is lobbying heavily for the bill's passage. Lynn Grefe, the association's president, thinks it represents the best possible intervention. "I'm excited about this," Grefe said. "If we can get this passed in New York, I'd work to get it passed all over the country."
There are efforts at the federal level, too. The Gail R. Schoenbach F.R.E.E.D Foundation and the Eating Disorders Coalition continue to advocate for the F.R.E.E.D. Act, an acronym for the Federal Response to Eliminate Eating Disorders Act, which seeks to fund research, and to improve the screening and diagnoses of eating disorders. The treatment section would require every insurance policy to cover eating disorders. The current law is full of loopholes. For instance, a policy may pay for therapy but not for a nutritionist. If a heart condition is the result of an eating disorder, insurance companies may refuse to pay for visits to a cardiologist. Additionally, the F.R.E.E.D Act requires treatment centers to follow the standard of care prescribed by the American Psychiatric Association, thus eliminating poorly managed facilities that do patients more harm than good.
No one knows how many people die from eating disorders annually, male or female. MacDonald noted that a coroner may conclude someone has died of heart failure, but fail to write that this occurred as a result of anorexia. The F.R.E.E.D Act's research section would fund "centers of excellence" capable of capturing more accurate and current data. These centers would also train educators in hopes of spreading knowledge.
Luckily, the F.R.E.E.D Act is a stand-alone bill. It is not attached to President Obama's hotly debated health care legislation. As states challenge the constitutionality of universal health care, passage of the F.R.E.E.D Act remains a viable possibility. At the end of 2010, the bill had the bipartisan support of fifty-one sponsors in the House and nine in the Senate. It was reintroduced in early 2011, and its advocates hope to bring it to committee this year. "I have never had anyone say, that's a stupid issue and I'm not planning on voting for it," MacDonald said. Although not specifically targeted at males, the F.R.E.E.D Act is an inclusive bill that attempts to aid both genders, all ages, and those who suffer from all manifestations of the disease.
Dr. Warren supports all legislative efforts to fight eating disorders, but does not think they go far enough. "I want the education to come from every direction – from patients, from families, from the media, from medical societies, from medical schools, everybody," Warren said. "I think if we can come at it from ten or twelve directions, we can have success. We're way better off than we were ten years ago. My prediction is ten years from now, we're going to be much, much happier with where things are at."
Ava can be contacted at

